COVID-19 : FORCED EVICTIONS
This Situation Report covers operational updates in countries where the Protection Cluster is active

Context update
COVID-19 is now reported in 213 countries, areas or territories around the globe (UN OCHA), and the WHO continues to rate the global risk as ‘Very High’. In our 32 countries of operation, the number of cases are rising since the last sitrep. Most operations suspect underreporting due to all, or a combination of, weak reporting systems, deliberate control of figures, lack of testing facilities, as well as testing costs, and growing stigma associated with COVID-19 among some communities.
Vulnerable populations continue to face barriers in accessing services, while humanitarian actors encounter obstacles in delivering them. This week a horrific attack on an MSF maternity ward took place in Afghanistan, killing babies, mothers and nurses in the capital Kabul. In the past weeks we have seen an increase in attacks against humanitarian actors in Central African Republic (CAR), fires displace vulnerable IDPs in Bamako, Mali, and flooding affect IDP hosting areas in Burundi, Yemen, Somalia, Philippines and Myanmar. Weather-related crises, from heat waves and drought to cyclones and floods, and subsequent food insecurity, are likely to hit countries already struggling with the pandemic in coming months, disaster experts have warned.
At its 921st meeting, the AU Peace and Security Council adopted a communique on the situation of IDPs, refugees, returnees, migrants and peacekeepers in Africa in the COVID- 19 context, and reiterated the UN Secretary General’s call for the global ceasefire.
National Protection Clusters are working to support a safe, dignified and inclusive response to the immediate health needs resulting from the pandemic, whilst also ensuring continuity of vital services for pre-pandemic needs and addressing the related protection and socio-economic consequences that will impact vulnerable populations. Through their extensive networks of cluster members and community networks, as well as increased effort to build the capacity of local leaders and community-based actors through remote training methods, National Clusters are able to reach IDPs, host communities and people most vulnerable to the pandemic where they reside.
Emerging Protection Trends
IN FOCUS: EVICTIONS
Even in non-pandemic times, displaced communities are highly vulnerable to eviction. Stigma, poverty, challenges earning sufficient funds to pay rent and utility fees, as well as difficulties claiming and exercising their rights, is witnessed in IDP evictions across contexts. These challenges are currently exacerbated by the economic downturn and loss of livelihoods experienced by many IDPs during the COVID-19 pandemic. As evictions of IDPs increases, measures to stop the spread of the virus – self-isolation, social distancing, and proper hygiene practices – are undermined. IDPs face few alternatives than to move in with relatives, or seek communal shelter options, where overcrowding makes transmissibility of the virus impossible to prevent. Evictions are especially dangerous for the elderly, children, people living with disabilities and underlying medical conditions.
In Colombia, even after the signing of the peace agreement in 2016, in the midst of the COVID-19 emergency, communities continue to be affected by the lack of security of tenure, with persistence of internal displacement and difficulties of return. Families who are victims of violence have to live in the outskirts of cities or in overcrowded population centers without access to essential services such as water, nor proper transportation services, among others. Evictions of tenants of less than 30 days have occurred, even within the framework of the Decree that prohibits them.In Iraq, evictions remain one of the key protection concerns for communities, with the latest protection survey suggesting people are sinking into greater debt as a coping mechanism. In Ethiopia, office closures due to COVID-19 have meant that people are unable to obtain birth registration and other civil registration documents that have a direct impact on their ability to access housing and land tenure. In Somalia, forced evictions represent a constant threat for vulnerable communities in the country, including displaced populations living in collective settlements and other urban poor in densely populated areas – the HLP AOR has successfully advocated for evictions moratoria in several jurisdictions in the country for the duration of the pandemic. For guidance on advocating for evictions moratoria, refer to this tool developed by the HLP AOR.
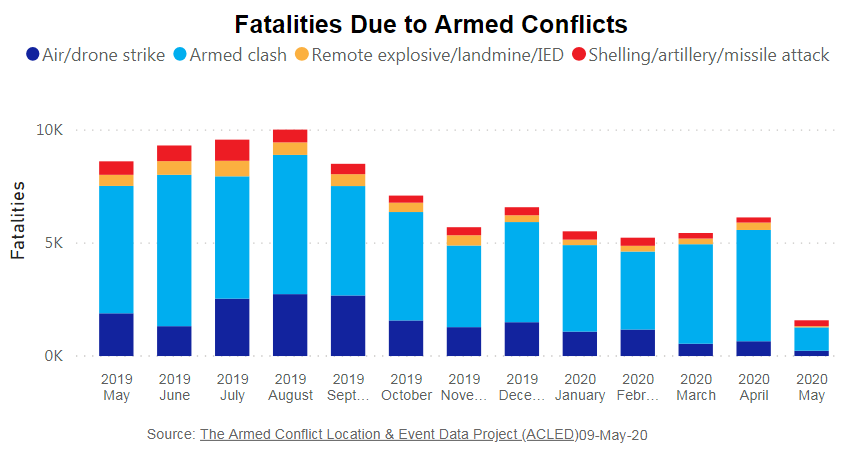
Conflict and COVID-19: Conflicts continue across the globe, with armed conflict steadily increasing since March. This ongoing violence is directly threatening the safety and health of millions and causing further displacement of communities. Conflict is also reducing safe access to vital health and sanitation services and reducing humanitarian access to those who need it.
- In Afghanistan a deadly attack on an MSF maternity ward left dozens of dead, including newborns, mothers and nurses. The Government has now declared a resumption of offensive operations against armed groups.
- The ceasefire has not been respected in Yemen with conflict continuing across the country, while the transmission rate of the virus is increasing.
- Attacks against humanitarian organisations including the killing of a humanitarian worker have increased in Central African Republic. The number of incidents per month spiked from one in January to nine in April.
- Continued fighting around the Lake Chad Basin resulted in cutting off of telephone and internet services across large areas, hindering communication and remote working modalities and making it difficult for humanitarian actors to track displacement, and implement the COVID-19 and protection response.
- In DRC, where they are still dealing with the Ebola crisis in the northeast of the country on top of the COVID-19 outbreak, there continues to be fighting between state and non-state actors in the east, triggering additional waves of displacement and hindering access for protection actors.
- 3 more hospitals were attacked in Libya, impeding the coronavirus response as well as breaching international humanitarian law.
- In Colombia, non-state armed actors are capitalising on the lockdown and reduced presence of the State to strengthen their control of certain areas. This is driving severe human rights violations, while reducing the visibility of risk situations, as risk monitoring by the State and humanitarian actors is hampered.
Discrimination and stigma: As the UN Secretary General warns of a ‘tsunami of xenophobia’, field clusters are reporting limited and discriminatory access to services, including health, across several operations, as well as stigmatization of people and communities accused of carrying the virus. Arbitrary and/or limited access to protection services and/or humanitarian assistance, which in turn exacerbates psychological distress, is reported across contexts.
- In Iraq, 38% of respondents from a recent protection survey report that none, or not all, of their community members have access to health care.
- There are increased reports of push backs of migrants trying to enter Libya from bordering countries, where they are facing discriminatory restrictions to healthcare.
- In Cameroon and Nigeria, forcibly displaced persons are at heightened risk of stigmatization, a situation exacerbated by fake news and misinformation. There is concern that this could result in politicization of the issue should displaced communities become heavily affected by the virus.
GBV: One in three women have been subjected to gender-based violence worldwide. With the threat of COVID-19 and its consequences, including restricted mobility, confinement, reduced community interaction and the closures of services, including support for those at risk or survivors of GBV, there is an increase in the risk of their exposure to GBV.
- GBV is particularly high in communities living under the control of gangs in Port au Prince and other big cities in Haiti. Access to these communities is difficult for humanitarian workers. Tensions arising from the Covid-19 epidemic might further isolate victims of GBV in these communities.
- In Somaliland, domestic abuse and violence against women is reportedly increasing.
- Protection helplines in Colombia have reported receiving increasing calls related to GBV.
Socio-economic downturn heightening risks: Curfews, lockdowns, and limitation of gatherings inevitably have a strong social and economic impact, such as loss of livelihood and isolation from family and other support networks, leaving vulnerable communities at a heightened risk of exploitation, such as trafficking in persons, child-labour and early marriage.
- In Iraq, in a recent survey conducted by the protection cluster and partners, 89% of respondents report loss of employment and/or livelihoods as the main impact of the crisis, followed by the lack of access to humanitarian services (58%); inability or difficulty in purchasing basic necessities (55%); lack of access to government services (52%); and inability and/or difficulty to pay rent (44%).
- In Libya, access to livelihoods and basic services is proving increasingly challenging for displaced populations, further raising their exposure to negative coping mechanisms.
Freedom of movement: Measures to prevent and combat COVID-19 such as restrictions on national and international movements is resulting in forced return and movement of people while at the same time, limitations on or discriminatory restriction to freedom of movement remain a major concern for people living in internal displacement camps and sites.
- With border closures in place for COVID-19, migrants travelling through Guatemala are getting pushed back from neighbouring countries, generating tensions between host populations and the authorities. The government deported over 2,300 people since 22 March to Honduras where registration and medical checks are conducted prior to transfer.
Children at risk: COVID-19 can quickly change the living environment of children. Measures such as the closure of schools, restrictions on population movements and social gatherings disrupt the social support for children and can put them at risk. The risks of family separations can increase (due to separation with primary caregivers who might fall ill, be quarantined, or displaced), as well as the risks of death of sick parents, even stigmatization and exploitation of children who survive them. Negative coping mechanisms such as early marriage, trafficking in persons and child labour are also a risk when families face socioeconomic hardship.
- Children can be separated from their primary caregiver(s) – because they are quarantined away from their primary caregiver or their primary caregiver(s) is quarantined and unable to care for their child. The wellbeing of children – particularly unaccompanied and separated children – is particularly at risk in quarantine facilities where child safeguarding measures are not available.
- Displaced children in DRC, many of whom now beg on the streets, are exposed to sexual violence, kidnapping, and economic exploitation. An additional concern is that they will not return to school because families now depend on the income generated by begging.
Abuse of power: Due to the COVID-19 crisis, individual and community protection capacities may be disrupted. There have been outcries over police brutality witnessed during their attempts to enforce lockdowns, and arbitrary confinement of returnees and migrants in quarantine centres, who have little access to humanitarian support.
- In Colombia the curfew has led to reports of extortion and harassment in many rural centres of the country.
- Use of excessive force against civilians is reported to be on the increase in Libya, to enforce curfews imposed by government around COVID-19.
- The limited access to monitor conditions of returnees and migrants in quarantine centres has been an issue reported across several clusters, including El Salvador, Guatemala and Venezuela.
Persons with disabilities: The pandemic has been devastating for the lives, health and well-being of older persons, people with underlying medical conditions, and those with lower socio-economic status – a category that tracks closely with minority status in most countries. The situation of persons with disabilities, especially those with underlying health conditions or in institutions, is particularly grave and it may be harder for them to access critical health care and take prudent steps to protect themselves.

Older persons have faced higher infection and mortality rates, while at the same time been subjected to ageism in public discourse, age discrimination in health care and triage decisions, neglect and domestic abuse at home, the effect of isolation on the physical and mental health of older adults, limited access to essential services, and greater exposure and poor treatment in care institutions.
IN FOCUS: Mozambique
Mozambique is a country that has been affected by various humanitarian emergencies over the past few years; it is just over a year since Mozambique was ravaged by two powerful cyclones which hit central and northern parts of the country and there are still more than 100,000 people who remain displaced from these disasters. In addition, the northern most Province of Cabo Delgado is facing a situation of violence in which 200,000 internally displaced persons are estimated while incidents of violence by unidentified armed groups continues to intensify and spread across the Province. Physical and safe humanitarian access to IDPs remains limited and the spread of the COVID-19 pandemic presents an emergency upon an existing emergency. Although relatively low number of cases of COVID-19 are reported in Mozambique, the Government has declared that the state of emergency will run through until the end of May. More than half of the confirmed cases of COVID-19 have all been concentrated in Cabo Delgado, which in turn has further reduced humanitarian access to displaced populations, both in terms of humanitarian actors having limited presence on ground, but also due to increasing incidence of violence. In Cabo Delgado, currently only 68% of health facilities are operational.
There are heightened protection concerns across the country, however particularly in Cabo Delgado where there has been ongoing violence since 2017. Protection actors are concerned about the risks posed to children in Cabo Delgado and in central parts of the country were many remain still impacted by last years disasters. Child friendly spaces for the time being are closed, and lockdown measures are keeping children out of school. In various locations in Cabo Delgado, IDPs are reported to be sheltering in schools without access to proper shelter facilities, others are being hosted by family and friends, which also increased the risk of COVID-19 contagion. Incidents of GBV are increasing and families often have to resort to negative coping strategies. There has been a reported increase of recruitment of children into unidentified armed groups operating in Cabo Delgado
In Central Mozambique, the Protection Cluster including AoRs have a set of protection focal points in IDP communities who are provided with mobile phones and will receive remote training and serve as key informants in highly vulnerable IDP sites, a model which the Protection Cluster aims to set up in Cabo Delgado as well. This activity is paired with Non-food items (NFIs)I distribution to pre-identified highly vulnerable individuals, including persons with disabilities, in coordination with the Shelter Cluster.
IN FOCUS: OCCUPIED PALESTINIAN TERRITORY
COVID-19 (C19) lockdown measures and restrictions in the occupied Palestinian territory (oPt) remain in place. Severe restrictions on movement throughout the West Bank, including East Jerusalem and Gaza have significantly curtailed protection related service provision. In Gaza there are formal quarantine centres and anyone arriving through Erez or Rafah crossing must complete is a 21-day mandatory quarantine. Whilst Israeli authorities announced in late March a moratorium on demolitions of inhabited buildings, important structures such as WASH and health points, and eventually also inhabited buildings, have been demolished, undermining efforts to contain the virus.
There is now an almost total absence of face-to-face interaction and access to life-saving gender-based violence and child protection services. Several GBV service providers in the oPt report an increase in the number of GBV cases and calls to hotlines have reached quarterly averages within weeks. Most concerning is the increasing reports of high risk cases including suicides and attempted suicide linked to domestic violence. For women, recently released from Gaza prisons as part of measures to ease overcrowding, there are concerns that some are returning to live with extended families in potentially difficult and hostile environments, without adequate protection measures in place and challenges for partners to conduct outreach to the households. Areas reportedly creating pressure and risks are delayed legal proceedings in Sharia courts, divorce, custody proceedings and disruptions to family mediation processes. In Gaza, there is a chronic lack of safe places and recreational areas for children. The disruptions and related mental health stressors increase risks to children such as anxiety, trauma, psychosocial relapse and risks of increased violence in the home. One cluster partner reported a 24 percent increase in calls from children in the past week, compared to the first three weeks in April.
Partners have developed virtual ways to reach people to ensure continuity and comprehensive protection services to address existing as well as emerging issues. GBV, CP and MHPSS providers are adapting their modalities to remote delivery, providing psychological consultations, expanding toll-free helpline services and rolling-out social media, radio and TV awareness campaigns, remote remedial education and recreational activities for children including to remote communities. An inter-Ministerial procedure has been developed for the safe referral and care of GBV survivors during C19 including for health care, testing, social services and quarantines that include essential protective measures. In Gaza protection cluster has been training staff working in quarantine centres on GBV, child protection and MHPSS prevention and response. Across the West Bank, organizations have provided psychosocial support to hundreds of families, including support to children and managing stress linked to COVID-19. CBO partners in East Jerusalem work as part of local emergency teams providing CP/MHPSS interventions for children exposed to increasing ISF violence. Efforts by legal aid providers led to a moratorium on demolitions (see above) and children detainees to be granted phone contact with their families.
There are also concerns about the lack of information on measures to protect the right to health of Palestinian detainees in Israeli detention, and of a possibly discriminatory treatment in considering detainees for release or alternatives to detention to reduce crowding. Continued detention and new arrests of children are a particular concern. Restrictions on detainees’ abilities to contact family and lawyers are another protection concern. Israeli Security Forces search and arrest operations with uneven COVID19 protection measures in place had been a concern at one point. Violence and damage to Palestinian property by settlers in the West Bank remains high despite movement restrictions.
Operational Challenges and Support
The overall operational context remains challenging. Restrictions on movement and access to communities, alongside communications difficulties is limiting the capacities to deliver services. In some areas, this has caused temporary suspension of activities. However, across the response, protection clusters are leveraging new technology, piloting innovative remote delivery solutions, and utilizing preexisting widespread community-based protection networks to ensure that minimum protection programming and service delivery are maintained and adapted in remote settings. Field Clusters across all operations are implementing a “minimum package’’ of protection activities that can be implemented despite COVID-19 related restrictions.
Key Highlights from the response:
- Iraq has produced an online interactive dashboard presenting the results of the first round of data collection through the Remote Protection Monitoring Tool.
- A hotline and early warning system is being developed in Mali to make sure communities are able to prepare and adequately reach safety should attacks be imminent.
- In the Philippines an online seminar on GBV was attended by over 1200 participants, with high participation from the Government and NGOs.
- In the Democratic Republic of Congo and Mozambique, community protection focal points and committees were provided with mobile phones and credit to undertake protection monitoring in IDP communities.
- In Yemen, they have done an analysis of people at risk, developed protection mainstreaming along with guidance on preparedness for partners in COVID-19, and a complaints and feedback mechanism.
- OPT developed guidance on mainstreaming disability in the response.
- South Sudan developed a briefing note on how to ensure a protection and human rights lens to a COVID-19 response.
- In Syria , the protection cluster developed Protection Mainstreaming guidance for quarantine facilities targeting all clusters
- In Sudan, the cluster developed an advocacy note on protection and human rights considerations in the COVID-19 response
Based on consultations with the National Protection Clusters, the GPC has synthesized ongoing and planned activities into a minimum package of support. This “Minimum Package” on COVID-19:
- Identifies critical activities to be implemented feasibly in all protection cluster operations.
- Aims to increase predictability and clarity for key stakeholders on what can be expected from NPCs/FPCs.
- Intends to foster sharing, learning and best practices across operations.
- Provides a framework of key protection actions for the country chapters of the Global Humanitarian Response Plan (GHRP), the revisions of country Humanitarian Response Plans and of National Peace and Development Plans.
Effective and safe, dignified and inclusive: guidance and advocacy including on quarantine centre and shielding measures, trainings and operational support
Protection monitoring and protection analysis: harmonized protection needs assessments and monitoring, regular situation reports, monthly protection briefs and analysis
Protection advocacy: advocacy messages and campaigns
Protection awareness raising activities and campaigns: rights awareness and information dissemination, culturally adapted and through appropriate channels
Protection service delivery: alternative modalities for case management, adapted referral pathways, community-driven protection, Individual Protection Assistance (IPA), including cash for protection, MHP
For other operations in the GHRP, the GPC – including the Areas of Responsibility and other expert organizations – offer to provide support based on requests in support of existing coordination structures. The support package includes the following options:
1. Introductory Training on Humanitarian Coordination, the Centrality of Protection, Human Rights Based Approach & Protection Mainstreaming.
2. Training on basic protection coordination tools. (Mapping of capacities, 4W).
3. Support for needs and risks identification and analysis.
4. Support to develop COVID-19 Protection Strategies to HCTs and/or Government counterpart and set up COVID-19 Field Protection Working Groups or other coordination platforms.
5. Support in designing specific protection projects, programmes and response modalities for the COVID-19 protection programming and monitoring the response.
6. Support Advocacy initiatives and information campaigns on COVID-19 response (common key messages and communication tools) including engagement with communities.
7. Support with specialized staff fully dedicated to the operation.
Humanitarian Response Plans and COVID-19 Plans
The May update of the Global Humanitarian Response Plan (GHRP) for COVID-19 was published last week. The GHRP was extended to 63 countries around the world, and financial requirements have risen from 2B to 6.7B USD, in addition to 30.1B USD adjusted requirements for non-COVID-19 humanitarian responses.
The GHRP includes 27 countries with active protection clusters, sectors or working groups responding to pre-COVID-19 humanitarian situations which have been revising and adapting their response to COVID-19 risks and impacts. The protection requirements for COVID-19 response in those operations amount to over 270M USD, in addition to 1.7B USD adjusted requirements for non-COVID-19 responses, taking the overall protection requirements to 2.0B USD.

Despite the criticality of protection to saving lives, the overall protection funding requirements for both COVID-19 and non-COVID responses represents less than 8% of total humanitarian requirements in those 27 operations. It is vital this small portion of the overall budget is met. The GPC is concerned historically poor funding trends will continue – in 2019, only 37% of protection requirements under HRPs were funded, and so far in 2020 only 6% has been received. We will continue to advocate for the criticality of protection funding for both COVID-19 and non-COVID humanitarian responses, to ensure that there is a critical operational footprint and that the needs, rights and appropriate responses for vulnerable groups are adequately championed within the response.
We have also noted a wide variation across countries regarding the relative weight of protection asks within total HRPs and COVID-19 requirements. Total protection requirements range from 20-30% in a few countries (Colombia, Iraq, Libya and Ukraine) to less than 5% in several others (Chad, Ethiopia, Mozambique, Philippines, Sudan, Yemen and Zimbabwe). This is largely explained by the difference in protection risks and needs, contexts, operational capacity / access, feasibility and overall conditions put in place by the humanitarian leadership. But is also due to differences in the representation of programmes dedicated to protection challenges that do not have designated Areas of Responsibility, including for addressing psychosocial support and trafficking in persons, as well as working with persons with disability, older people and youth. We will be working with clusters and partners towards better harmonization of protection responses, targets and requirements in the upcoming planning processes, in particular, in the HPC 2021.
For more information or queries, please contact the GPC COVID/19 Advocacy lead, Dorothy Sang dorothy.sang@oxfam.org.
| The Global Protection Cluster is a network of NGOs, international organizations and UN agencies, engaged in protection work in humanitarian crises including armed conflict, climate change related and natural disaster. The GPC ensures well-coordinated, effective and principled protection preparedness and responses, and that protection is at the core of all humanitarian action and recognized as essential in any nexus with development and peace. The GPC unites members, partners and communities working on the full gamut of protection activities, including in four specialized Areas of Responsibility: Child Protection, Gender-Based Violence (GBV), Housing, Land and Property and Mine Action. The GPC contributes to and benefits from the broader IASC system. |

